In late March, a paraplegic patient in China stood up and took steps through intentional control. Not in the clean, abstract way a demo video usually frames these things, but through a messy clinical stack: a brain-signal cap, spinal cord stimulation, an exoskeleton, repeated training, and a patient who still hopes that one day he can walk with a cane instead of living in a wheelchair.
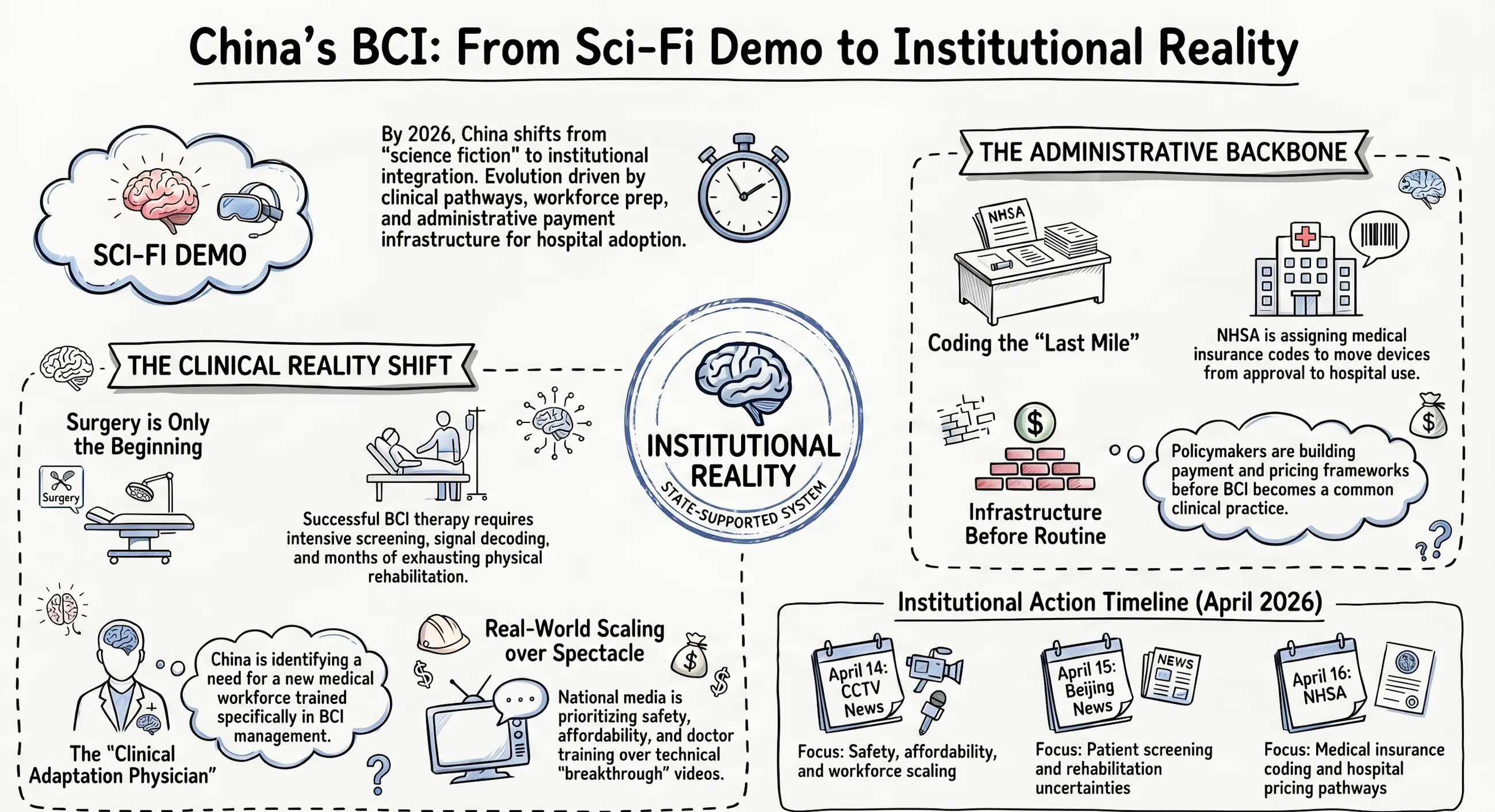
On its own, that would still be a striking medical story. What made April 2026 feel different was what happened around it. On April 14, CCTV’s News 1+1 segment on brain-computer interfaces treated the field not as science-fiction spectacle but as a public question: how safe is it, how expensive is it, how do you scale it, and who is going to train the doctors? On April 15, a long Beijing News / Shell Finance feature showed how much patient screening, rehabilitation, and uncertainty still sit behind each visible “breakthrough.” On April 16, the National Healthcare Security Administration (NHSA) pushed the discussion into a different register altogether: coding, pricing items, hospital charging pathways, and the mechanics that decide whether a frontier device remains a headline or becomes something the health system can actually absorb.
That is why China’s BCI story now looks more consequential than a run of eye-catching lab milestones. The shift is not simply that the technology looks more futuristic. It is that, for the first time, it is beginning to look institutionally real.
From demo to clinical pathway
The easiest mistake is to read these cases as proof that the hard part is over. The reporting suggests almost the opposite. Beijing News described a patient at Tongji Hospital who, after a spinal cord injury, used a non-invasive brain interface, spinal stimulation, and an exoskeleton to complete a standing-and-walking trial. The article also described another cluster of cases around Beijing Tiantan Hospital’s implanted BCI work, where patients are screened, tested for signal quality, and then pushed through a long rehabilitation process in which “implant” is only the beginning.
That distinction matters. Much of the popular imagination still treats BCI as if the device itself is the therapy: put it in, switch it on, and function comes back. The April reporting points to a harsher reality. Patients need to qualify. Signal quality needs to be good enough. Rehabilitation takes time. Training is exhausting. Expectations need to be actively managed because many patients arrive hoping for a dramatic reversal and are told instead that they may be entering a long experimental path with uncertain payoff.
The CCTV segment made the same point from another angle. In its discussion of the implanted system known as Bei Nao-1 (北脑一号), clinicians emphasized that the surgery is only the start. Patient and device have to adapt to one another. Doctors have to understand not just neurosurgery, but decoding, training, expected response, and the practical rhythms of clinical use. That is already a very different stage from a university press release. It suggests China is moving from “can this be shown?” toward “what would it take to run this as care?”
Why the CCTV framing matters
National television is not a scientific validation mechanism, and it should not be confused with one. But what it chooses to foreground still tells you something about where a technology sits in public life.
The April 14 CCTV discussion did not frame BCI mainly as a futuristic curiosity. It framed it as a social and institutional problem set. Safety came first: surgeons said the first nine Bei Nao-1 implant surgeries had not produced serious complications so far, and that signals remained stable and clear. Affordability came next: even if surgical fees may end up looking similar to other implant procedures, the device itself is still expensive and early-stage. Then came scale: can this become something more than a handful of high-profile cases? Finally came workforce: clinicians explicitly discussed the need for a new kind of “clinical adaptation physician” for brain-computer interfaces, because conventional medical training does not quite cover what this field now needs.
That framing matters because it moves the conversation away from raw technical prowess and toward system capacity. A technology becomes more real, in the public sense, when the questions stop being “is this possible?” and start being “who pays, who trains, who manages risk, and what counts as a good enough outcome?” CCTV’s treatment suggests that BCI in China is crossing that line. It is no longer just a story about whether engineers can decode a signal. It is becoming a story about whether institutions can carry the burden of making that signal useful.
This is also where China may have a structural advantage. The clinicians interviewed by CCTV argued that the country combines strong top-down policy coordination with a large patient base and fast clinical feedback loops. That does not guarantee good outcomes, and it certainly does not remove the risks. But it does help explain why the conversation is now moving so quickly from lab performance to hospital process.
The real signal is payment infrastructure
The most important development in this April cluster may not be any single patient story or even the nationally televised surgery. It may be the fact that the payment side is starting to prepare for BCI as a category.
The NHSA’s April 16 article was unusually revealing because it focused on what many technology narratives skip: the administrative plumbing. In the Chinese healthcare system, price items and medical insurance coding (医保编码) are not glamorous, but they are the difference between “approved” and “usable.” A device can be technically impressive and even formally approved, yet still stall if hospitals do not know how to charge for it, how to code it, or whether the broader payment system can recognize it at all.
That is why the earlier NHSA note from March 22, 2026 mattered so much. It said that after the world’s first approved invasive BCI product reached the market, the agency moved quickly to assign a medical insurance code, explicitly presenting this as a way to bridge the last mile from approval to clinical use. The April 16 piece pushed the same logic further, arguing that China is no longer dealing only in isolated technical advances but is beginning to assemble a full path from research to approval to charging and, potentially, reimbursement.
That is a bigger signal than it may first appear. In many frontier-medtech stories, the heroic moment is regulatory approval. In reality, approval often just opens the door to the next bottleneck. Hospitals still need a way to purchase, bill, and justify adoption. Payers still need categories, codes, and some framework for deciding whether a device belongs inside ordinary medical finance or outside it. The NHSA’s recent language suggests Chinese policymakers understand this very clearly. They are not waiting for BCI to become routine before designing payment pathways; they are laying down some of that infrastructure early.
This may turn out to be one of the most distinctive features of China’s BCI push. The country is not only trying to produce technically credible systems. It is also trying to shorten the gap between invention and institutional uptake. That does not mean the economics are solved. It means the system is at least attempting to solve the right problem.
Promising, but still early
None of this should be mistaken for mass adoption. The clinical evidence base is still thin. Long-term safety and stability remain open questions, especially for implanted systems. Real-world outcomes may end up more modest than early narratives suggest. Rehabilitation burdens are heavy. Patient selection is strict. Costs are still high. And if BCI moves beyond a narrow set of severe neurological indications, the ethical questions around data, autonomy, and access will become harder rather than easier.
There is also a subtler risk: overreading institutional motion as proof of mature utility. A government can create codes. Hospitals can open clinics. Broadcasters can spotlight success cases. None of that, by itself, proves durable patient benefit. The field still has to answer the most basic medical question: does the intervention produce enough functional gain, for the right patients, at an acceptable risk and cost?
Still, April 2026 does seem to mark a change in texture. China’s BCI story is no longer just a lab story, and not merely a venture-capital story either. It now has clinics, public scrutiny, and the beginnings of a payment path. That combination does not make the technology ordinary. But it does make it harder to dismiss as pure spectacle.
The most interesting thing about China’s BCI moment, then, is not that it feels like science fiction. It is that it is beginning to look like something hospitals, doctors, and the payment system might one day be able to carry together.